招待講演: lecture ”forehead lift for Japanese”
■ Figure 02
(Figure 02)
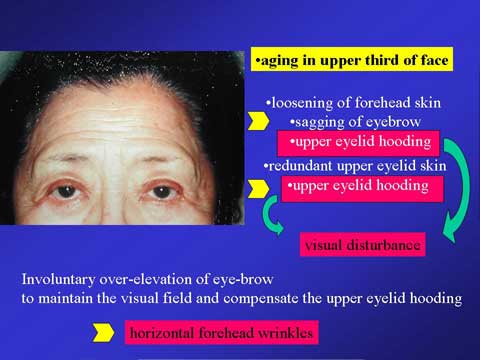
The aging of forehead develops loosening of forehead skin from the skull. This causes the sagging of eye-brow. The sagging eye-brow exaggerates intrinsic sagging of upper eyelid due to the loosening of double fold line or stretched skin.
The hooding of upper eyelid disturbs the visual field. Therefore, involuntary contraction of frontalis muscle takes in place; this action elevates the eye-brow and also lifts the sagging upper eyelid to improve the visual field. The over-contraction of frontalis muscle produces the horizontal wrinkles in the forehead. Thus, horizontal wrinkle is recognized as a typical aging sign of forehead. Another aging change could be realized as the sagging of the brow and upper eyelid, in case the over-contraction of the frontalis muscle did not take in place.
■ Figure 03
(Figure 03)
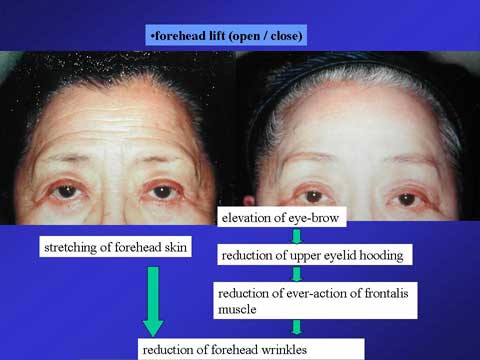
The purpose of the forehead rejuvenation is correction of the eye-brow sagging or reduction of forehead wrinkles, especially horizontal ones.
We have already known both open coronal and endoscopic brow lifts are effective. The brow (forehead) lift procedure can stretch the forehead skin itself, making the wrinkles smooth out. The lift procedure elevates the eyebrow, which correct sagging upper eyelid. This improves the visual field; thereby, the over-elevation of eyebrow is no longer necessary. As a result, the horizontal wrinkles which are related to the frontalis muscle contraction will disappear.
■ Figure 04
(Figure 04)
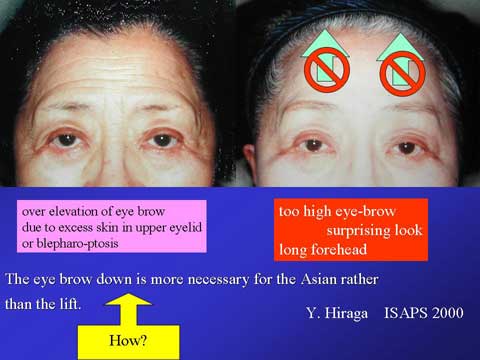
Thus the forehead lift procedure is very useful in case of eye brow sagging with or without horizontal wrinlkles. This aging problem is common in Caucasians. Many of Japanese patients, however, present with involuntary over-lifting of the eyebrow to elevate the upper eyelid and maintain the visual field.
The eyebrow lift procedure for those Japanese patients further elevates the eyebrow, which has been already high in position. Elevated brow is one of the aging signs for Japanese, Korean and Chinese. The brow lift further elevates the eyebrow, which make the patient look old or show a surprise look. The eye brow down is more important for the Asian than the lift. I totally agree with this idea.
■ Figure 05
(Figure 05)
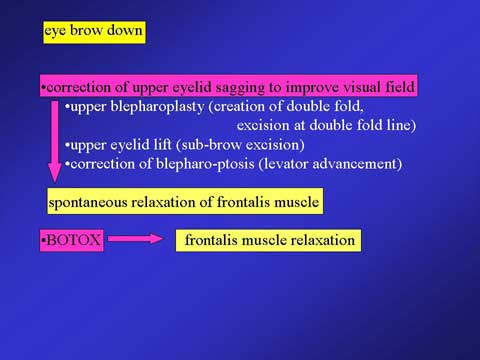
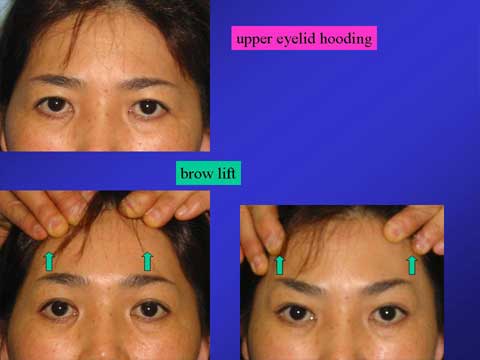
In order to make the brow down, it is necessary to relax the frontalis muscle. BOTOX is one of the solutions. Another approach is correction of sagging upper eyelid, improving the visual field. This decreases the involuntary contraction of the frontalis muscle. The procedure to correct the upper eyelid sagging includes blepharoplasty (double fold creation) in case of loosening double fold line and absent double fold line. Incisional blepharoplasty with skin excision has to be used if the skin excess is significant. In case of blepharo-ptosis, levator shortening procedure needs to be combined with blepharoplasty. The upper eyelid lift procedure performed by excising the excess skin at the sub-brow region is also very effective to bring the elevated eye-brow down.
■ Figure 06
(Figure 06)
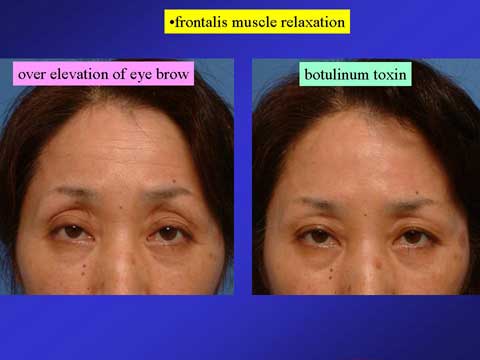
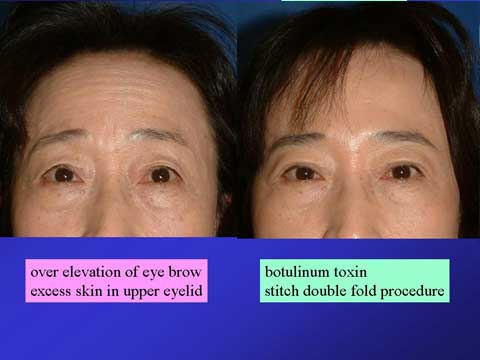
To eliminate horizontal wrinkles, injection of botulinum toxin A may be a treatment of choice. However, we must be careful in patient’s selection. In a good candidate for Botox treatment, sagging of upper eyelid should not occur.
■ Figure 07
(Figure 07)
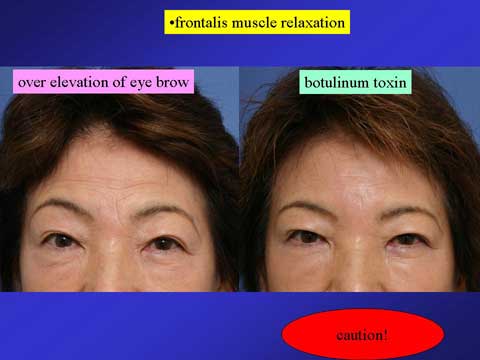
If the patient has excess skin in the upper eyelid, she may complain of narrow double fold or sagging of eyelid like this case. This could be a mistake of the patient selection.
■ Figure 08
(Figure 08)
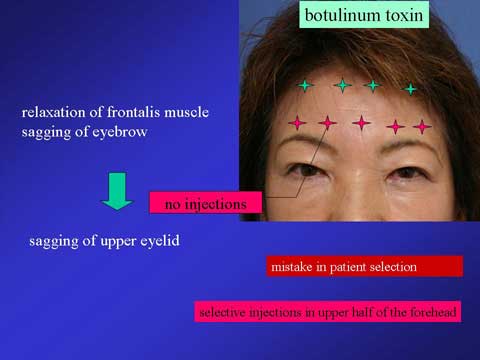
We should not treat this type of patient with BOTOX or should give the BOTOX only in the upper half of the forehead, leaving the lower portion of frontalis muscle in action. In this way, of course, horizontal wrinkles disappear only in the upper forehead. The wrinkles remains just above the eyebrow.
■ Figure 09
(Figure 09)
It may be helpful to perform upper blepharoplasty, such as stitch double fold procedure, at the time of Botox injection; this can reduce the hooding of upper eyelid after BOTOX treatment.
■ Figure 10 11 12 13 14
(Figure 10)

(Figure 11)
(Figure 12)

(Figure 13)

(Figure 14)

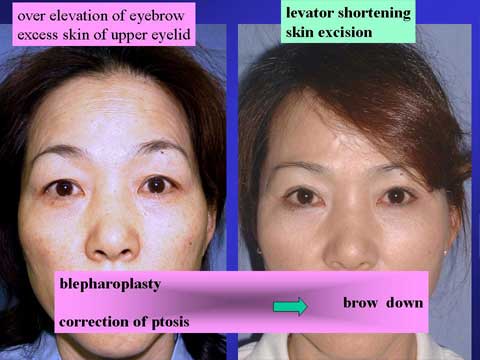
Good candidates for Botox injection may have blepharoptosis or sagging of upper eyelid; this may be the reason why they are elevating the eyebrow and making horizontal wrinkles. For those patients, the correction of upper eyelid problem helps to reduce the horizontal wrinkles without BOTOX treatment.
■ Figure 15 16
(Figure 15)

(Figure 16)
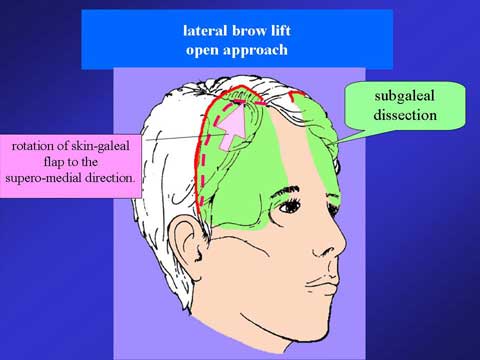
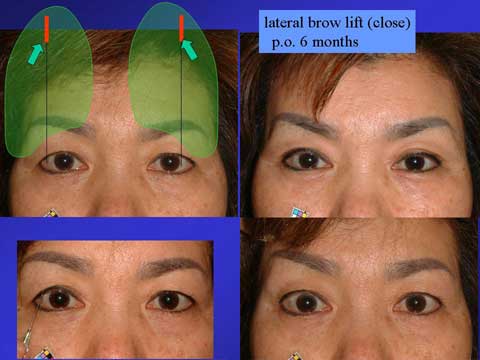
In case of sagging eyebrow, my approach is lifting the eyebrow mostly in the lateral portion. I make a hemicircle incision in each side of temporal region. The incision can be this long or shorter. I dissect under the galea over the periosteum. I rotate the flap supero-medially; this really elevate the lateral eyebrow.
■ Figure 17 18 19 20 21
(Figure 17)

(Figure 18)

(Figure 19)
(Figure 20)
(Figure 21)
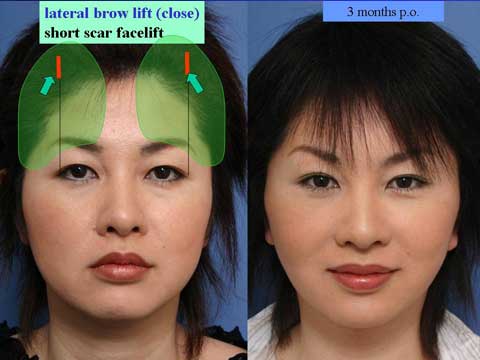
The lateral brow lift can be perfomed with long incision in the hair-baring skin of the temporal region or very short incision in the lateral forehead like an endo-lift.
■ Figure 22
(Figure 22)

In case of long forehead, the hairline incision can be used. I perform the subcutaneous dissection and skin excision along the hairline, preserving the suproirbital nerve in layer of frontalis muscle and galea
■ Figure 23 24 25 26
(Figure 23)
(Figure 24)

(Figure 25)

(Figure 26)
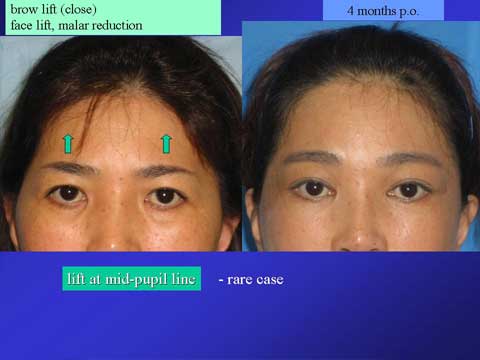
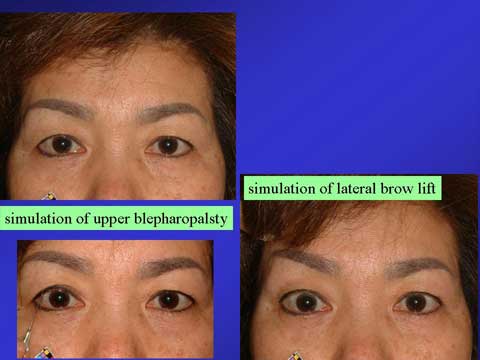
Elevation of the lateral portion of the eyebrow is useful in most of cases; however, the elevation of entire brow is necessary in limited cases. This must be determined in the presurgical planning.
■ Figure 27
(Figure 27)
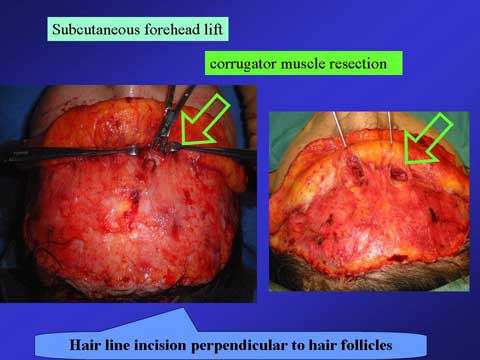
I use subcutaneous dissection plane on top of the frontalis muscl for forehead lift surgery to erase wrinkles. I make an incision along the hairline. I use a knife in a beveled fashion perpendicular to hair follicles. I tried to cut the hair follicles. I dissected the subcutaneous plane and split the frontalis muscle to expose the corrugator.
■ Figure 28
(Figure 28)
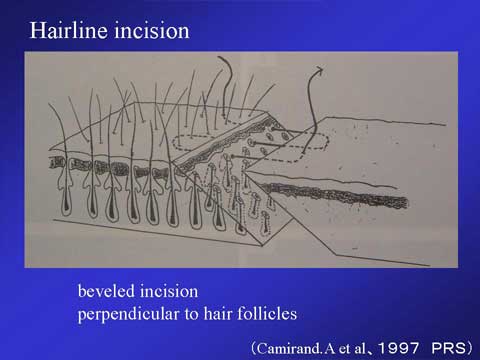
Beveled incision along the hairline was reported by Dr. Camirand on PRS in 1997. This remaining lower portion of hair follicles can grow hair through this advanced non-hair-baring skin.
I will demonstrate the the subcutaneous forehead lift in a video presentation. I use a knife in the beveled fashion about 30 degree to cut the hair follicles to make a hairline incision . I dissect in a subcutaneous plane, leaving the frontalis muscle intact on the skull. I split the frontalis muscle longitudinally at the bottom of the forehead between the supratrochlear nerve and supraorbital nerve. I dissect out the corrugator muscle and grab the corrugator with a hemostat and remove the muscle. I pull the skin flap gently, not trying to elevate the eyebrow in this case. I make just enough tension to eliminate the skin wrinkles. When I excise the excess skin, I use a knife in the beveled fashion again. The skin wound is closed in two layers.
■ Figure 29
(Figure 29)

This 72-year-old lady presented with significant wrinkle lines in the forehead and around the orbit. I performed the subcutaneous forehead lift through the hairline incision. 3 months after surgery, hairs grow through the scar and also non-hair-baring skin. The scar is well camouflaged.
■ Figure 30 31
(Figure 30)

(Figure 31)

This 63-year-old lady was concerned of her forehead wrinkles. Her upper eyelid show mild ptosis. When she closed her eyes and relaxed the frontalis muscle, her forehead wrinkles decreased but did not disappear. If I correct her blepharoptosis, she could get this much of improvement. In order to eliminate her horizontal wrinkles, I performed the levator shortening and subcutaneous forehead lift at the same time. This is one month after surgery. 3 months after surgery, she has no wrinkle in the forehead. The scar along the hairline is hardly seen in the forehead. The scar in the temporal hairline was also well camouflaged.
■ Figure 32
(Figure 32)

This lady presented with many fine wrinkle lines in the forehead and glabella. The elevation of the her upper eyelid is sufficient in the medial and middle portion of the iris. Opening of the lateral portion is not strong enough; this may give her tender look but also tired look. Her eyebrow looks low in position.
The levator shortening procedure may lower her eyebrow, which is already too low, therefore, I performed the levator shortening and subcutaneous forehead lift.
In summary, for the case with sagging brow or orbital hooding, I like to elevate the lateral portion of the eyebrow. It is important to consider the upper eyelid which may be a cause of forehead wrinkles.