
韓国美容外科アカデミー鼻の整形外科研修コース part2 2010/9/11-12
2 correction of bulbous tip; management of skin envelop
Keizo Fukuta, M.D.
Verite clinic, Tokyo Japan
Polly beak deformity is post-rhinoplasty deformity associated with fullness in the supratip.
Two categories of a Polly beak deformity are generally described; cartilaginous source and soft tissue source.
The letter category is more common in Orientals and more difficult to correct.
The nasal skin in many of Oriental patients is thick and inelastic, providing poor redraping after reduction rhinoplasty such as correction of bulbous tip.
Excess of thick skin and soft tissue develops at the supratip region.
We have used direct skin excision in a spindle shape overt the supratip bulkiness.
This simple procedure can remove the excess soft tissue and convert the bulging dorsal contour to straight line.
Only problem concerned after this method is a postoperative scar on the nasal dorsum.
10 Japanese patients were treated with the direct excision.
The scar became inconspicuous in 3 cases without further treatment and in 7 cases after CO2 laser abrasion.
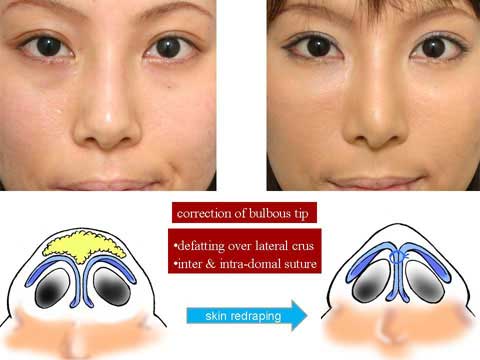
The correction of bulbous tip, making the tip narrow and sharp, is a common request for Oriental rhinoplasty.
The correction can be done using endo-nasal incision by removing subcutaneous fat tissue from the regions over the lateral crura of alar cartilage and between the bilateral middle crura and approximation of cephalic marign of bilateral lateral crura.
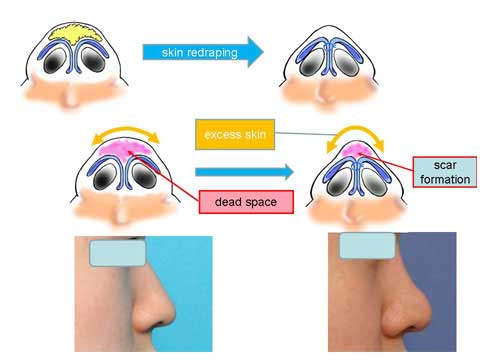
Why does Polly beak deformity occur? When we perform the defatting and cartilage suture, we expect that the skin should redrape nicely over the modified cartilagenous structure.
In case the skin is soft and pliable, it will do so.
However, those who ask for bulbous tip correction, their skin tends to be thick and hard. The nice redraping does not take place.
Therefore, the dead space from wide subcutaneous dissection can not be eliminated, causing scar tissue formation.
Excess amount of skin will bulge out when it is squeezed in the midline.
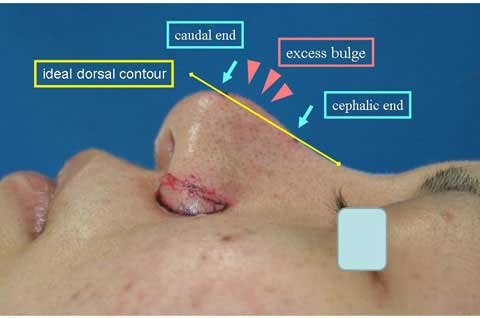
A case with Polly beak deformity after having undergone the correction of bulbous tip.
Here in my imagination, I extend a dorsal contour line in straight.
This line helps me to find the caudal end and cephalic end of the excess bulge.
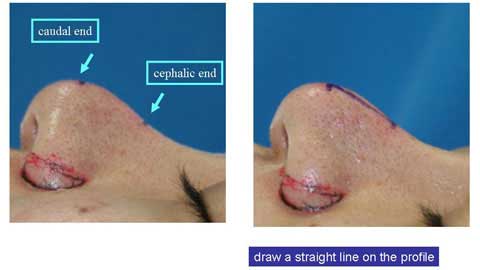
I draw a straight line from the cephalic end point to the caudal end point on the profile.
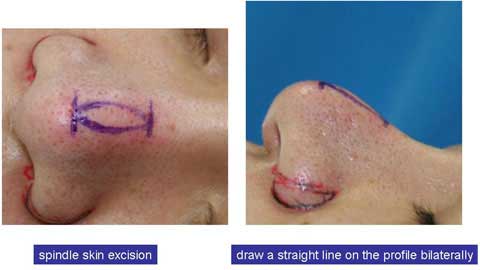
I draw another line on the other side.
When we look from the front, those straight lines are not really straight but slightly curved.
We can actually see a marking of spindle shape.

I excised full thickness skin of the spindle mark and closed the defect in two layers.
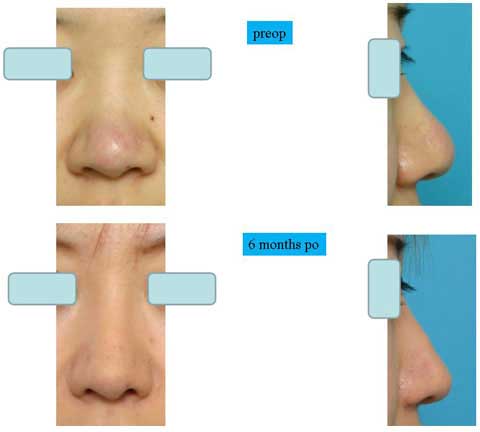
These are the patient before surgery.
This is the result 6 months after skin excision.
The bulging of the supratip region became flat, even concave. The scar is inconspicuous.
In summary, spindle skin excision is very effective to correct Polly beak deformity.
Although this procedure leaves a scar, the scar is well accepted by patients.
Actually the scar was almost invisible in some cases.
This procedure was found useful not only for postoperative Polly beak deformity but also for primary bulbous tip.
The amount of skin excision should be conservative in width, otherwise it will result in concave contour or dog ear deformity.