
第7回韓国鼻美容外科シンポジウム、ソウル 2010/6/27
特別講演-Special lecture
Personal Philosophy of Septal Extension Graft for Asian Nose
発表内容-Announcement contents
Personal Philosophy of Septal Extension Graft for Asian Nose
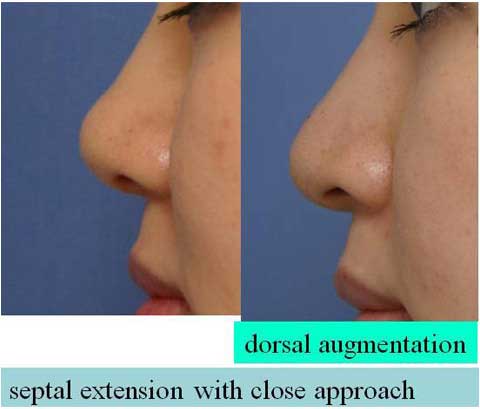
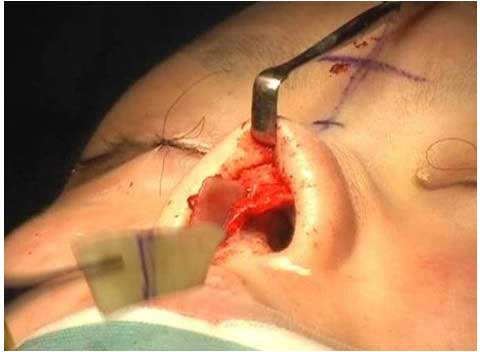
My standard approach for the septal extension graft is open rhinoplasty.
It would be preferable to use endo-nasal approach from the patients’ point of view because the close rhinoplasty avoid visible scar.
I have used open approach as long as a patient accepts the transcolumellar incision.
In fact, 90% of my patients accepted the open approach. Only 10% of my patients strongly requested the close approach.
The difficulty in close approach is limited visualization and narrow access for graft insertion due to the small nostril opening in Oriental nose.
In case of a large nostril opening or case with combined alar reduction, the close approach is slightly easier.
For the close approach, I use bilateral infra-cartilaginous (IF) incision with medial extension along the columella down to the columella base.
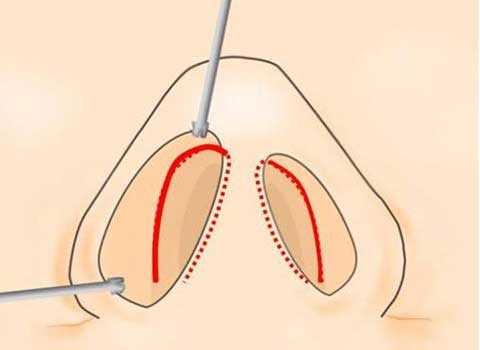
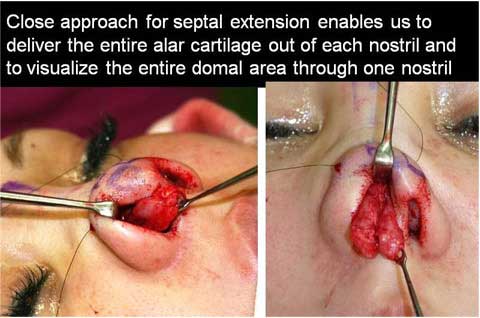
This 10 mm extension of incision gives a great mobility of alar cartilage, making it possible to deliver the entire alar cartilage out of each nostril.
In addition, delivering the bilateral alar cartilage in one side of nostril, the entire domal area can be visualized through one nostril.
Dissection between the medial crura and septal cartilage can be performed under direction vision.
The insertion and fixation of extension cartilage graft is cumbersome.
I had to convert the close approach to the open approach in 2 cases because of fear of breaking the thin graft or thin caudal septum in situ.
Although I fixed the alar cartilage to the extension graft under direct vision, it was difficult to achieve bilateral balance, avoiding the deviation.
Advantage of the close approach is no visible scar.
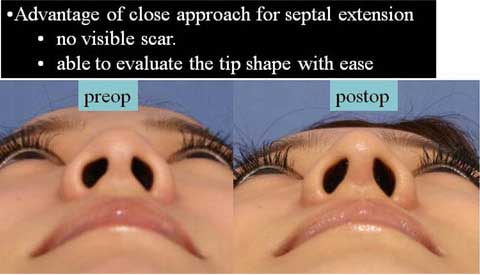
In addition, we can evaluate the tip shape with ease.
The open approach requires the closure of the transcolumellar incision each time when the tip contour is to be checked.
Disadvantage of the close approach is difficulty in fixation of the extension graft to the caudal septum and control the tip and columella position in the midline.
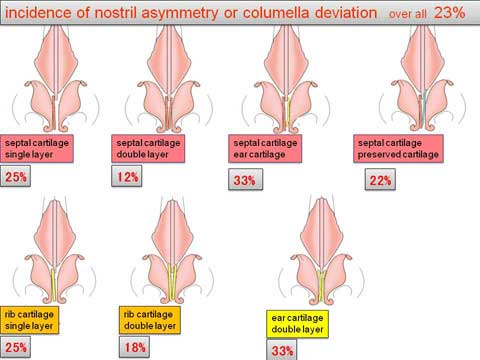
Although it is difficult, the incidence of asymmetry or deviation was 18% with close method and 23 % with open method in my experiences.
The above mentioned disadvantage results from the small size of nostril in our population. I think that patient selection is important to make a surgeon’s life easy.
As my experiences with septal extension graft have increased, I have found postoperative problems related to this procedure no matter whether the approach used is close or open.
The most common problem is deviation of tip and columella.
Other complications include improper direction of extension, under-extension or over-extension of the tip and airway obstruction.
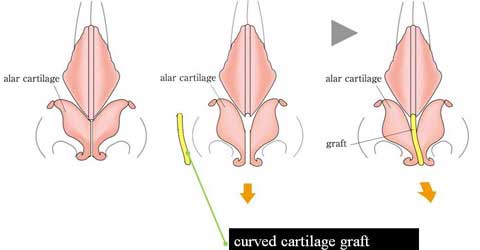
Causes of deviation are curved cartilage graft; week pliable cartilage graft, week pliable caudal septum in situ, deviated septum in situ, and unbalanced tension in bilateral advancement of alar cartilage due to previous scarring are potential cause of deviation.
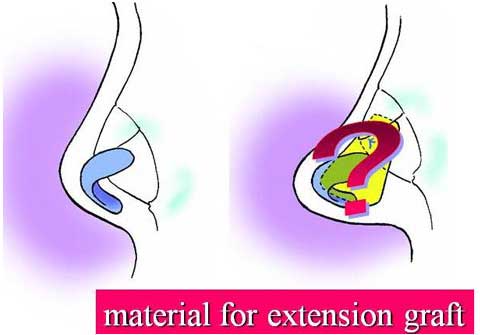
It is important to choose the adequate donor site for cartilage graft.
For last 2 years I performed septal extension graft on 153 cases.
I used septal cartilage for 76 % of my patients.
I chose costal cartilage graft for 17 % of my patients.
I used ear cartilage primarily for 5 %. For last 1 year, I have used preserved costal cartilage in addition to the septal cartilage graft for the reinforcement of mechanical support if necessary.
The preserved cartilage has been used in 26 cases, which were about half of the cases with septal cartilage graft for last 1 year.
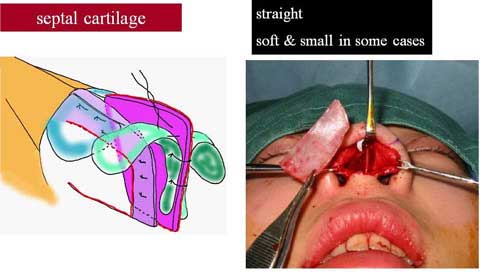
The septal cartilage is relatively straight and flat.
This is why I choose the septal cartilage for the first choice of graft.
However, the size of the graft available was not predictable until it was harvested.
In 4 of 153 cases, the septal cartilage graft was found too small, so I had to us ear cartilage as an extension graft.
The other 4 cases in which the ear cartilage was used had a history of septal excision.
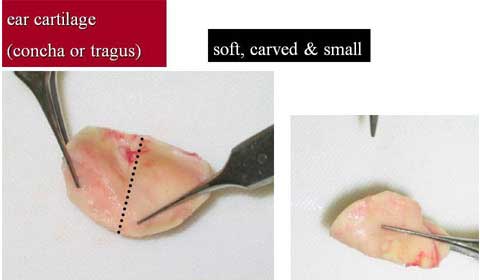
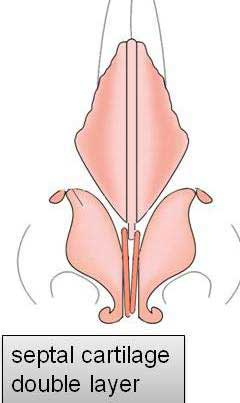
When I used ear cartilage for extension, I put the two pieces of graft together with multiple sutures.
Nonetheless, the two layered graft is not completely straight or flat.
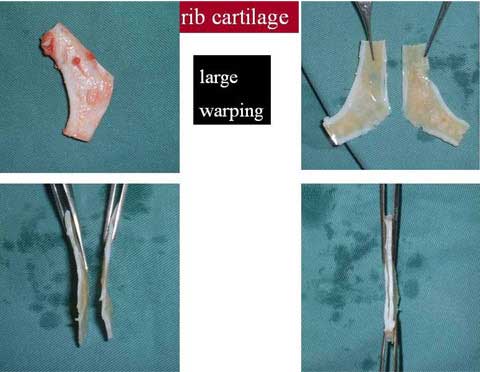
In case of costal cartilage, warping often develops after slicing the harvested cartilage.
It is not easy to obtain a straight graft material from the rib cartilage.
Two sheets of curved costal cartilage must be sewn together to adjust the curvature.
 |
figure 2: |
 |
figure 3: |
 |
figure 4: |
Even though we can achieve straight flat cartilage graft, it does not solve the deviation problem.
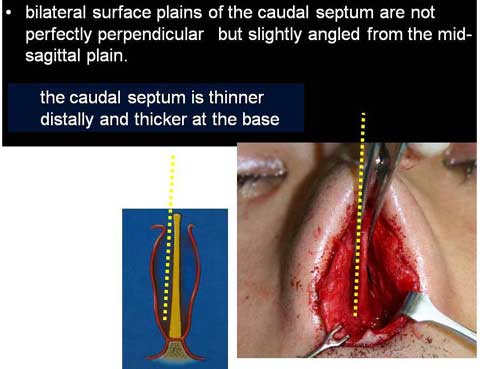
The bilateral surface plain of the caudal septum is not perfectly perpendicular but slightly angled from the mid-sagittal plain because the thickness of the caudal septum is not uniform.
The caudal septum is thinner distally and thicker at the base.
When the cartilage graft is fixed to the either side of the caudal septum, the fixed graft is accordingly deviated from the mid-sagittal plain, although the graft is straight and flat.
Therefore, it is necessary to fix two pieces of cartilage graft to the septum bilaterally and suture them together with great care to control the deviation.
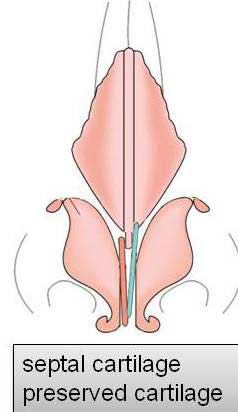
If the septal cartilage harvested is not large enough to produce two pieces of graft with secure tip support, I use preserved costal cartilage for one side.
The caudal and forward extension of the preserved cartilage should be smaller than those of the autologous cartilage graft on the other side.
In this way, the relapse of elongation will be avoided even though the preserved cartilage absorbs in the future.
Insufficient under-extension could be due to the limited size of cartilage graft.
It is essential to choose the donor site which can provide adequate quality and quantity of graft material.
The other cause of under-extension is tight mucosal lining.
The tight skin envelop may result in under-extension, but this case has been rare in my experiences.
In my experiences, the correction of under-extension is very difficult.
It required a large and strong cartilage graft such as costal cartilage.
Even the adequate cartilage was used, the postoperative course was often complicated with infection or deviation.
Over-extension or inadequate direction of extension occurred due to surgeon’s mistake in the intraoperative judgment or surgeon’s error in aesthetic sense.
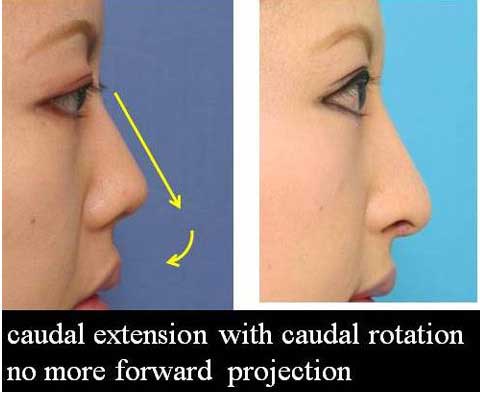
The common problem I have seen is unwanted forward projection of the tip
Another mistake I have noticed is undesirable de-rotation of columella.
Although the surgeon’s wrong sense of beauty is the cause of this result, it develops in case of missing extension support near the columella base.

This likely occurs when a surgeon uses narrow long bar type of extension graft, such as extended spreader graft.
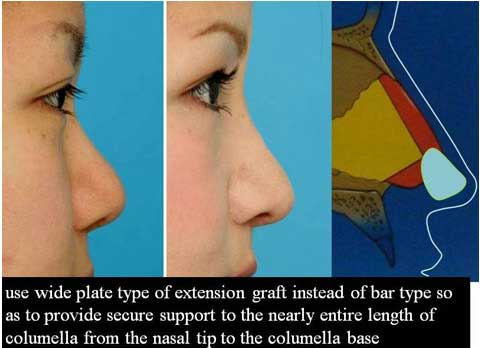
Therefore, I would like to use wide plate type of extension graft instead of bar type so as to provide secure support to the nearly entire length of columella from the nasal tip to the columella base.
Other unwanted result was excess columella show or exaggerated upper arched nostril.
It is important to take into consideration the position and curvature of nostril rim and to adjust the amount of caudal extension to less extent.
Shortening of extended tip or re-direction of extension is a relatively safer procedure compared with the correction of under-extension.
Even though a surgeon performed a proper extension, increase of extension, shortening of extension of re-direction of extension are requested from the patients when the patients change their mind postoperatively or recognize the results different from their preoperative expectation.
Airway obstruction is not common; it was found only 2 % of patients in my series.
The airway obstruction took place due to narrowing of the internal valve.
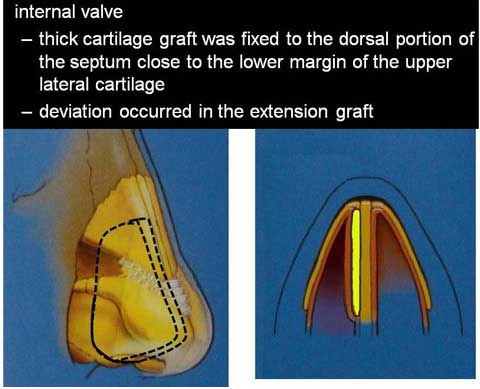
In case thick cartilage graft was fixed to the dorsal portion of the septum close to the lower margin of the upper lateral cartilage, the internal valve became narrow.
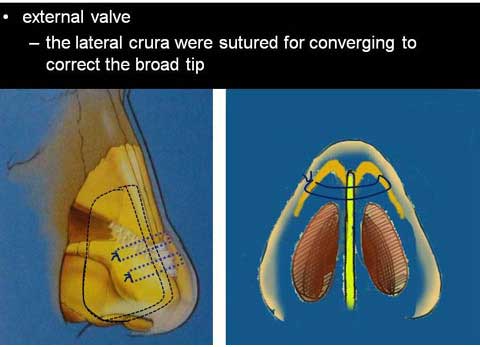

It also became narrow when the lateral crura were sutured for converging to correct the broad tip.
If the deviation occurred in the extension graft due to soft tissue tension, the obstruction could be worse.
This type of airway problem can be corrected by trimming of the grafted cartilage adjacent to the internal valve.
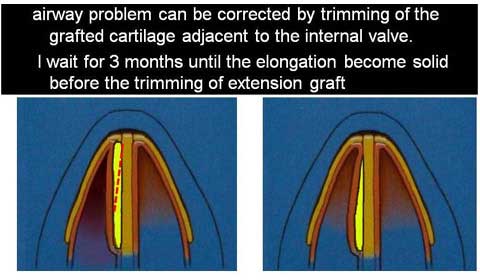
I wait for 3 months until the elongation become solid before the trimming of extension graft.