
第14回国際整鼻術ワークショップ、ソウル、韓国 2010/11/7
Problems in alar reduction and their management
Keizo Fukuta, M.D.
Verite clinic, Tokyo Japan
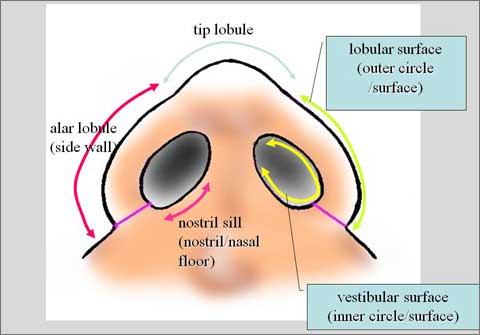

It is important to determine where the excess tissue exists and select the excision site (either side wall or nasal floor or both) according to the nostril shape.
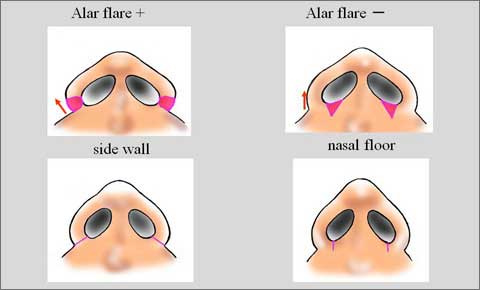
The side wall should be excised in case of alar flare.
The nostril floor has to be reduced for non-flare type.
Wrong selection of excision site results in unnatural deformed nose such as side wall excision for non-flare type.
In contrast, excision of the nasal floor for flare type results in increased alar flare. Although the site of excision is correct, over-excision produces a disaster.
Postoperative deformities in alar or nostril are notching of the nostril sill, excessive narrowing of the nostrils, flat alar side wall and asymmetry of the nostril.
These distortions occur due to inadequate alar reduction. In addition, excessive dome suture technique can cause extreme narrowing of the nostril with sharp angulation at the anterior corner.
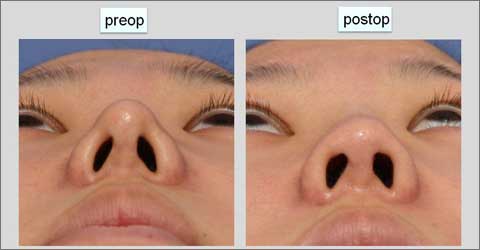
The lecture presents my experience with correction of surgical appearing nostrils.
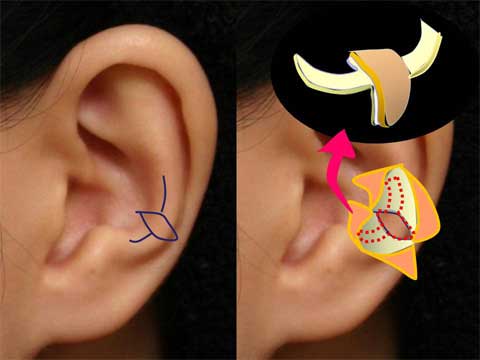

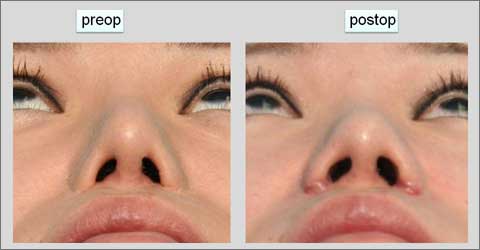
I use a composite graft to correct notching or stenosis of the nostril sill.
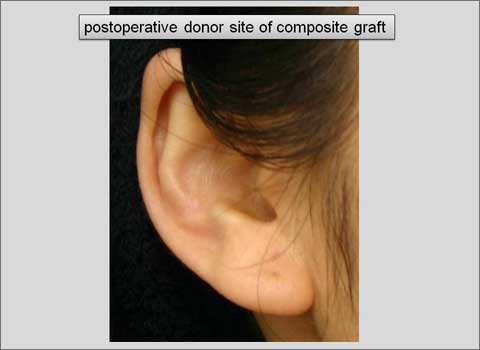
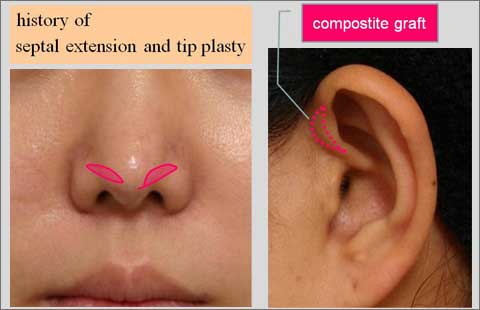
A composite graft is harvested from the antihelix of the ear.
The graft has a spindle skin island with underlying cartilage and two arms of cartilage extension.
Notching corner of the nostril sill is cut and opened.
Two subcutaneous pockets are made medially and laterally just beneath the vestibular skin.
The cartilage arms are inserted into the pocket and spindle composite island is placed in the opened space.
This type of the composite graft is helpful to provide the alar side wall with flare.

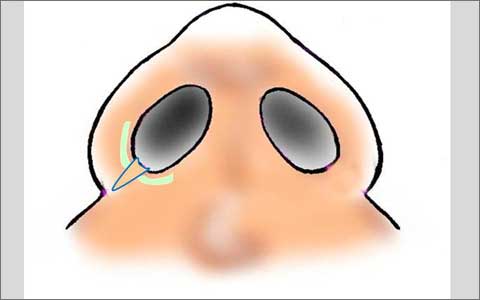
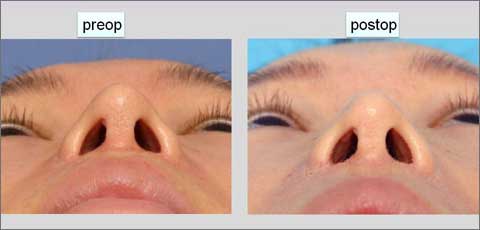
The narrow nostril with acute angle at the anterior corner is also treated with composite graft.
An incision is made caudal margin of the lateral crus.
Dissection above the cartilage allows the caudal and lateral advancement of nostil rim.
A spindle shaped composite graft is harvested from the inner surface of the crus of helix.
The graft is placed in a defect of the vestibular lining.




The flat alar side wall can be corrected with rim cartilage graft.
A strong curved cartilage piece is placed in the subcutaneous pocket in the alar side wall. The cartilage graft is harvested from the triangular fossa or cymba of concha.
Surgical techniques and clinical results are shown in the lecture.